
Impact of Health Education in Promoting Disease Preventative Behaviors Among High School Students
- Pre-Collegiate Global Health Review

- Nov 4, 2022
- 10 min read
Divya G. Tadanki, Milton High School, Milton, Georgia, USA

Abstract
Health education is a common state-mandated requirement for students in primary and secondary education levels. However, the existing literature has found conflicting evidence on the effectiveness of health education in disease prevention, and much of the literature excluded high school students from middle-class communities. The purpose of this study was to discern whether school health education achieves its purpose of promoting disease preventative behaviors, specifically among the high school age demographic. The hypotheses predicted a positive correlation between the completion of the health education requirement and the development of hygienic behaviors, as well as a difference in the behaviors between those who have and have not completed the course. Upon a correlational analysis, Z-Test, and thematic content analysis of the surveyed results from 100 participants in Georgia, it was found that there is no significant relationship between the variables. The lack of statistically significant results on the habits of those who have and have not met the Georgia-mandated health requirement indicates that health education is ineffective in this population. This suggests that new and improved health education curricula that are adapted to the students’ maturity level and psychological state should be implemented in order to improve the effectiveness of the health education system in the urban and suburban regions of Georgia and the urban regions of the United States.
Introduction
The World Health Organization defines health education as “learning involving some form of communication designed to improve health literacy, including improving knowledge, and developing life skills which are conducive to individual and community health” (WHO, 1998). Forty-six U.S. states require health education for all grade levels, and in Georgia, high schoolers are required to complete one unit of health education.
Disputes on Health Education Effectiveness:
A 2015 study on hand hygiene interventions among elementary school-aged students did not reduce the prevalence of gastrointestinal and respiratory infections or reduce illness-related absences (Willmott et.al, 2015). Another study on reproductive health education contradicts these findings. Researchers found that skill-based intervention initiatives improved the attitudes, knowledge, and practices of the students in this rural region of India where certain health topics were heavily stigmatized (Phulambrikar et al., 2019). An oral health intervention program was similarly successful in improving student knowledge of dental hygiene and reducing oral-related health issues in participating students (Harikiran & Nakre, 2013). A common theme is that—when implemented appropriately—health education can help children manage their personal health. However, the strong disputes among experts in the field warrant further study into the topic.
Topics for Further Exploration in the Body of Knowledge:
Despite the breadth of health education research, there are gaps within the body of knowledge. This research aims to prioritize three of these gaps: audience age, health topic, and surveyed location. Many existing studies focus on elementary school children, so those results cannot be generalized to high school students due to differences in psychological development and maturity. Much of the research also revolves around different areas of health education, so this study prioritizes school hygiene education. Lastly, many health education studies focus on underdeveloped countries or rural areas. The circumstances of children in these environments are not applicable to those living in more suburban regions within the United States. Therefore, the research question of this study is: how effective is health education in improving disease preventative behaviors among suburban high school students?
Hypotheses:
The hypotheses of this study–based on existing literature discussed later in this paper— are stated below:
H0: There is no statistically significant correlation between health education and the development of disease preventative behaviors among high school students.
H1: There is a statistically significant correlation between health education and the development of disease preventative behaviors among high school students.
H2: There is a statistically significant difference in the practices of disease preventative behaviors between those who have and have not completed a health course.
Methods:
A 2017 study from the Journal of Family Medicine and Primary Care entitled “Impact of school health education on personal hygiene among school children of Lucknow district” explored the effectiveness of health education on a group of elementary children in India (Khatoon et al., 2017). Researchers used a cross-sectional study, using pre-tests and post-tests to assess knowledge among children between the ages of 6-12. In this region, health education improved children’s understanding of hygiene practices (Khatoon et al., 2017). Another study on “Person hygiene among college students in Kuwait” also employed a cross-sectional study to compare differences in male and female hygiene habits (Al-Rifaai et al., 2018). These studies were the basis for this research, and the questionnaires used in these papers were used in this study.
Participants:
The sample for the study included 100 students, aged 14 - 18, from a high school in Georgia. Sampled students were also members of school clubs that imposed GPA requirements. This was done to control variances in academic motivation. Participants received one service hour for a club upon completion of the survey.
Materials:
The study was conducted after being approved by an Institutional Review Board (IRB). All participants were required to submit informed consent forms (Appendix A) before participating. All identities were kept anonymous, and participants were able to withdraw at any time. Students could opt out of answering questions, although this option was not utilized.
A survey distributed electronically was used due to its ease of use and accessibility. Respondents answered a series of Likert-scale or free response questions. Survey questions (Appendix B) were from the CDC Health Education School Questionnaire, the Journal of Education and Health Promotion questionnaire, and the Journal of Family Medicine and Primary Care questionnaire.
Procedure:
An experimental study—as used in the existing works– could not be implemented, as there is no way to control which students have already received health education. In the studies cited above, students had no access to health education, which allowed for an experimental study. However, the difference in the U.S. environment means that some students may have already taken a health course prior to the mandated state curriculum course. By using a correlational study, confounding variables were limited.
Measures:
The independent variable was the completion or incompletion of the high school health requirement. The dependent variable was the healthy habits practiced. Data from those who have completed high school health education and those who have not were compared against one another.
Results:
Demographics:
Of the 100 students that participated in the survey, 70% were between the ages of 16-17, 17% were in the 14-15 age group, and 13% were 18.
82% of participants identified as female and 16% as male, with the remaining 2% identifying as another gender. The distribution of racial groups was as follows: 48% white, 42% Asian, 3% Black or African American, and 7% other.
Quantitative Data Results:
Figure 1 below shows the relationship between the perception of the effectiveness of hygiene education and the frequency with which hand hygiene habits are practiced. The x-axis indicates a Likert-scale representation of how effective students perceive health education to be in improving hand hygiene, with a rating of 1 being not effective and a rating of 5 being very effective. Similarly, the y-axis also uses a Likert scale, showing the frequency with which students practice healthy hand hygiene habits. A rating of 1 indicates very infrequent hand hygiene and a rating of 5 indicates very frequent hand hygiene. A correlational analysis yielded an R-value of –0.0054434. For comparison purposes, a significance value of r=0.4 was used. The computed R-value indicates that there is no relationship between the two variables.

Figure 1: Correlation of health course and hand hygiene habits.
A second correlational analysis on a student’s ranking of the quality of knowledge on disease preventative practices gained from a health education course and the frequency of hygiene habits practiced was employed.The x-axis shows a student’s Likert-scale ranking of the quality of knowledge on disease preventative behaviors they have acquired from a health class. A ranking of 1 indicates a low quality of knowledge and a ranking of 5 indicates a high quality of knowledge. The y-axis indicates the frequency with which students practice healthy hygiene habits, with a rating of 1 indicating very infrequent hand hygiene practice and a rating of 5 indicating very frequent hand hygiene practice. Figure 2 below presents a graphical interpretation of the data collected. The computed R-value, 0.017, once again indicates that there is no significant relationship between the variables.
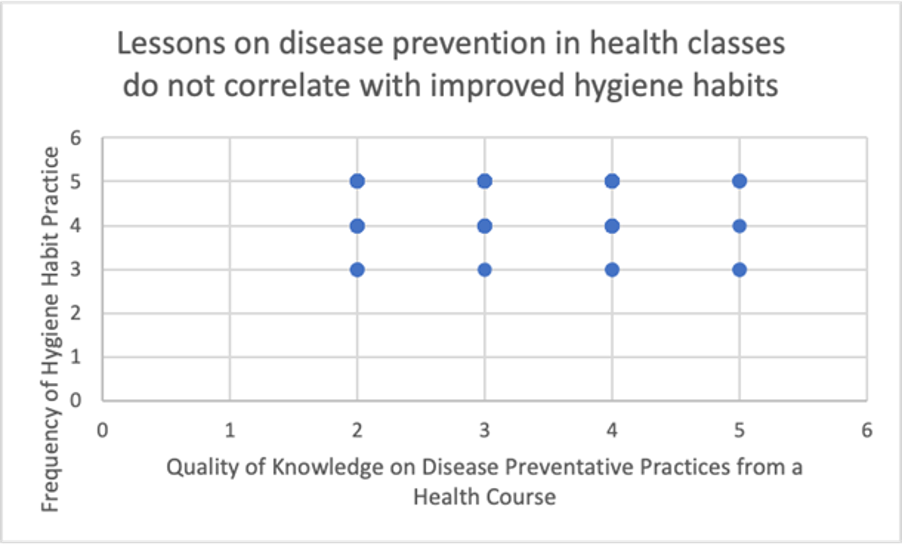
Figure 2: Correlation of lessons on disease prevention and hand hygiene habits.
A third statistical analysis method was also used. By utilizing a 2-sample Z-Test for Proportion, it was possible to discern if there was a significant difference between those who completed a health course and practice hygiene habits and those who have not completed a health course and practice hygiene habits. The blue-colored bar shows the proportion of students who completed a health course and practice healthy hygiene habits, while the orange-colored bar shows the proportion of students who did not complete a health course and practice healthy hand hygiene habits based on survey responses. This analysis yielded a p-value of 0.53, which falls above the significance level of 0.05. The overlapping error bars in Figure 3 and the large p-value indicate that the null hypothesis mentioned earlier cannot be rejected.

Figure 3: Proportion of students practicing healthy hygiene habits.
Qualitative Data Results:
Students that completed a health course were asked to elaborate on their views on the school health education curriculum. Figure 4 shows that 18.7% of respondents reported that health education had no effect on their habits, while 17.6% reported that it improved their habits. However, the statistical analyses presented earlier in the 2-sample Z-test for p show that that value is not statistically significant. Furthermore, 20.8% of participants described health education curricula as forgettable and inapplicable in their daily lives, with 9.9% stating that health sources outside of the health education curriculum are more useful in promoting hygiene. Furthermore, 6.6% of participants felt that the health curriculum disregards external factors that may influence health, such as intrinsic motivation. 12.1% of respondents also reported that the health curriculum is too repetitive year to year, and 3.3% of respondents also felt that the curriculum censors topics that are more important. There was some inconsistency in students’ remarks on the breadth of the curriculum, with 6.6% stating that it is too broad and 4.4% stating that it is too narrow.

Figure 4: Common themes in student views on health curriculum.
In order to understand how the COVID-19 pandemic affected hygiene habits, students were asked to describe how the pandemic affected their hygiene behaviors. The results are detailed in Figure 5. 82% of respondents reported that COVID-19 improved their habits, while a smaller group of 16% reported that it did not impact their habits and 2% reported that it worsened their habits. This data supports the data presented in Figure 4, as there appears to be a link between outside health sources relaying COVID-19 information and improved hygiene habits.

Figure 5: Relationship between Covid-19 and Hygiene Habits
Discussion
The research indicates that there is no significant correlation between health education and the development of disease preventative behaviors. There also is no statistically significant difference in the practices of hygiene behaviors between those who have and have not completed a health course. The null hypothesis was not rejected because both R-values were close to 0.
In the inferential statistical analysis, a p-value of 0.53 was calculated, which did not meet the significance level of 0.05. Therefore, the null was not rejected.
These results are further supported by the qualitative data collected. Many students reported that the health curriculum was forgettable, inapplicable, and repetitive, stating that external information was more important in promoting hygiene. Additionally, responses on the role COVID-19 played in hygiene habits found that COVID-19 improved hygiene habits due to increased health information from news sources and medical professionals. While health education may not affect hand hygiene, resources from the media and medical professionals can affect hygiene behaviors.
Based on this evidence, health education and hand hygiene behaviors do not correlate with one another.
As these findings contradict those in the body of knowledge, this study provides reason to further analyze health education in first-world nations. Further comparisons between the hygiene habits of students in urban areas and rural areas are necessary to understand how different demographic groups respond to health education.
Discrepancies with Existing Research:
This study contradicts the existing literature, where health education appeared to positively impact students’ understanding and practice of hygiene habits in India and Kuwait (Al-Rifaii et al., 2018; Khatoon et al., 2017). This can be attributed to the socioeconomic differences between the participants in these studies. The cornerstone research was conducted primarily in developing nations, while this study was conducted in an upper-middle-class region of the United States. It can be deduced that the social context of the student plays a significant role in the effectiveness of health education (Hahn & Truman, 2015). The socioeconomic climate of India and Kuwait is not comparable to the United States, where 88.9% of the population has access to the appropriate resources to practice hygiene habits (Al-Rifaai et al., 2018; Khatoon et al., 2017; Mueller & Gasteyer, 2021).
Additionally, the differences in the age groups among participants may have resulted in the findings varying from previous work. High school students may respond differently to the health education curriculum or have already developed the appropriate behaviors, unlike elementary students.
Limitations:
Because the results rely on a convenience sample, the study has its limitations. Not all ethnic and socioeconomic backgrounds were represented in the study, so the sample is not representative of the diversity of students from this region of Georgia and urban areas in the United States. Demographically, the participants were between the ages of 14-18, with many participants identifying as female and the main racial groups being white and Asian. The results can only be generalized to those similar to the participants in this study. Additionally, because only 9% of the sample had not completed a health school in their high school career, data is lacking on the hygiene habits of those in this category. Selecting participants for the study through random sampling and increasing the sample population beyond one school would improve this study.
Implications:
Based on qualitative and quantitative results from the study, it can be inferred that health education curricula in high schools may be unable to effectively promote disease preventative behaviors in students. Hence, new techniques and a curriculum applicable to today’s youth should be adopted. Incorporating a more modern curriculum with more complexity for each additional age group could potentially create health education programs that effectively promote disease preventative behaviors, amongst other health benefits.
Future Work:
Studying the relationship between behaviors outside of hand hygiene and health education can provide a more nuanced understanding of the effectiveness of health education.
Additionally, conducting a two-sample study with students in urban and rural high schools can provide a basis for comparison of how health education effectiveness varies among different groups. While this study focused on a high school in a suburban region, expanding the study to include students from other regions will help determine if the health education curriculum should be adapted to a student’s environment.
References
Al-Rifaai, J., Al-Haddad, A., & Qasem, J. (2018, July 6). Personal hygiene among college students in Kuwait: A health promotion perspective. Journal of Education and Health Promotion. doi: 10.4103/jehp.jehp_158_17 Centers for Disease Control and Prevention (n.d.). Health education state questionnaire. https://www.cdc.gov/healthyyouth/shpps/2000/questionnaire/pdf/hltheds2000questionnaire.pdf Harikiran, A., & Nakre, P. (2013). Effectiveness of oral health education programs: A systematic review. Journal of International Society of Preventive & Community Dentistry, 3 (2), 103-115. doi: 10.4103/2231-0762.127810 Khatoon, R., Sachan, B., Khan, M., & Srivastava, J. (2017). Impact of school health education program on personal hygiene among school children of Lucknow district. Journal of Family Medicine and Primary Care, 6 (1). doi: 10.4103/2249-4863.214973 Phulambrikar, R., Kharde, A., Mahavarakar, V., Phalke, D., & Phalke, V. (2019). Effectiveness of interventional reproductive and sexual health education among school going adolescent girls in rural area. Indian Journal of Community Medicine, 44 (4), 378-382. doi: 10.4103/ijcm.IJCM_155_19 Tyack, David. (1992). Health and social services in public schools: historical perspectives. The Future of Children Journal, 2 (1), 19-31. https://doi.org/10.2307/1602459 Willmott, M., Nicholson, A., Busse, H., MacArthur, G., Brookes, S., & Campbell, R. (2015). Effectiveness of hand hygiene interventions in reducing illness absence among children in educational settings: A systematic review and meta-analysis. The British Medical Journal, 101 (1), 42-50. doi: 10.1136/archdischild-2015-308875
Appendix A
Consent Form to Participate in a Research Study Researcher’s Name(s): Divya Tadanki Project Title: Effectiveness of Hygiene Health Education in Improving Hygiene Practices Among High School Students INTRODUCTION This consent may contain words that you do not understand. Please ask the researcher to explain any words or information that you do not clearly understand. Your child is being asked to participate in a research study. This research is being conducted as part of an AP Research class. When you are invited to participate in research, you have the right to be informed about the study procedures so that you can decide whether you want to consent to participation. This form may contain words that you do not know. You have the right to know what your child will be asked to do so that your child can decide whether or not to be in the study. Your child’s participation is voluntary, and your child does not have to be in the study if the parent or child objects. Your child may refuse to be in the study and nothing will happen. If your child elects not to continue the study, he/she may stop at any time without penalty. WHY IS THIS STUDY BEING DONE? The purpose of this research is to investigate the relationship between hygiene health education provided in schools and the improvements in hygiene habits among high school students. This study aims to discern if health education in schools is achieving its purpose in promoting student health and healthy lifestyles in the students who are in the health classes. HOW MANY PEOPLE WILL BE IN THE STUDY? About 120 people will take part in this study through Milton High School. WHAT AM I BEING ASKED TO DO? Your child will be asked to answer a series of questions, which vary in response type. Some questions are Likert-Scalar (strongly agree, agree, …), and others are free-response questions (describe your reason for choosing…). Your child will respond to questions pertaining to their personal health, hygiene habits, and the health education they have received thus far in their high school career. HOW LONG WILL I BE IN THE STUDY? This study will take approximately 15 minutes to complete. During this time, your child will respond to the survey questions (multiple choice) and free-response questions (no word limit). Please allow for a minimum of 15 minutes in order to accurately respond to the questions. WHAT ARE THE BENEFITS OF BEING IN THE STUDY? Your child’s participation will help us understand how effective health education is in promoting health and student well-being, particularly in high school students. With this research, we will be able to understand whether the health education curriculum needs to be altered or reformed in order to protect students and inspire them to take control over their personal health. WHAT ARE THE RISKS OF BEING IN THE STUDY? The study will take place entirely virtually, through the use of Google Forms; thus there is no risk of violating CDC COVID-19 guidelines in contracting or spreading the disease. CONFIDENTIALITY Your child will be asked to specify their name, gender, age, race, and grade, as well as questions about their wellness and health. This information will not be shared with anyone, and neither will any of the survey answers be matched to names or distributed to the public. If your child chooses to stop participating at any time in the study, all stored information (pre-survey responses, questions, survey responses) with your child’s participation will be discarded. WILL I BE COMPENSATED FOR PARTICIPATING IN THE STUDY? Your child will receive no payment for taking part in this study. However, your child may receive 1 point of volunteering for the Honors Societies they are active members in. If doing so, please be sure your child completes the appropriate question on the questionnaire and contacts the officers of the relevant organization to ensure the point is received. The researcher of this study is not liable if the student does not receive a service point for any of these organizations for participation in this research study. WHAT ARE MY RIGHTS AS A PARTICIPANT? Participation in this study is voluntary. You do not have to participate in this study. You may be informed of any new information discovered during the course of this study that might influence your health, welfare, or willingness to be in this study, especially related to COVID-19. WHO DO I CONTACT IF I HAVE QUESTIONS, CONCERNS, OR COMPLAINTS? Please contact 770-365-6101 or divyatadanki@gmail.com if you have questions about the research, and your role as a participant. Feel free to ask questions when the research is complete as well. A copy of this Informed Consent form will be given to you before you participate in the research. SIGNATURES I have read this consent form and my questions have been answered. As a volunteer, my signature below means that I do want to be in the study. I know that I can remove myself from the study at any time without any problems. As a parent/legal guardian, my signature means that I have given consent for my child to participate in the study. Volunteer Date Parent/Legal Guardian Date
Appendix B
Preliminary Questions
Name:
Age: Race:
American Indian or Alaska Native
Asian
Black or African American
Native Hawaiian or Other Pacific Islander
White
Other
Gender: How do you identify?
Female
Male
Non-Binary
Prefer to self- describe:
Prefer Not to Disclose
Grade:
9th
10th
11th
12th
Have you completed a high school-based health class?
Yes
No
If yes, please indicate the year in which you completed the course.
9th grade
10th grade
11th grade
12th grade
Did you complete the course through a virtual platform (FVS, GAVS) or in person?
Virtually
In-person
NA
Do you currently have a pre-existing health condition?
Yes
No
How often do you get a health checkup?
Once in 3 months
Once in 6 months
Once a year
Only when needed
Never get it done
Other
Likert Scale Questions: Personal hygiene is about general body cleanliness.
Strongly Agree
Agree
Neutral
Disagree
Strongly Disagree
My health class helped me comprehend concepts related to disease prevention.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree I feel that the health education curriculum provided me with the skills to access valid health information.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I am able to use goal-setting skills to enhance my personal health.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I feel the health education curriculum has a significant positive impact on my physical health.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree Please briefly elaborate on your answer above.
Free Response
The health education program provides communities with ample information on disease prevention.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I am able to advocate for my personal health.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I believe I have access to the necessary resources to practice personal hygiene (soap, water, hand sanitizer).
Strongly agree
Agree
Neutral
Disagree
Strongly disagree When I wash my hands, I do so with water and soap for 20 seconds.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I always use hand sanitizer to clean my hands if I am not able to access soap and water.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I always wash my hands with water and soap after using the restroom.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I shower or bathe a minimum of three times per week.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I wash my hands before I eat a meal.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I brush my teeth twice per day every day.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
We do not need to wash our hands when there is no visible dirt.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
I believe that my school treats health education as a priority.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
How effective do you perceive health education to be in improving your health habits?
Very effective
Somewhat effective
Neutral
Ineffective
Very ineffective
In your opinion, how effective would the following actions be to improve your hygiene practices? Check all that apply.
Community leaders and school staff support and openly promote hand hygiene.
Educational facilities make the resources for hand hygiene readily available.
Hand hygiene posters are displayed as reminders in educational facilities.
Each student receives annual education on hygiene practices.
To what extent has the Covid-19 Pandemic affected your hygiene and health habits? (ie. Have hygiene announcements affected your behavior? Did you start practicing healthier habits once the pandemic began?) (Free response)



I'm Jefferey Vargas. My girlfriend ended our relationship for seemingly no reason and I came to understand that my financial struggles may have contributed to this, as a healthy relationship is difficult without money and aside from God, having more money is often seen as vital. For spell expertise, Lord Meduza is the right person to turn to. My girlfriend left me for another man due to my financial situation but after connecting with Lord Meduza he created a spell that not only brought my girlfriend back but also made me a lottery winner of €116 million by providing me with the 6 lucky numbers to play the lottery. Everything feels almost unreal but I assure you this is genuine…